

by Diane Rufino, April 7, 2019
This past week, NC house representatives in Raleigh addressed one of the biggest ideological battles of this legislative session – does government work for the taxpayer or for special interests, and the answer has come back to us loud and clear —- the NC House works for special interests, namely, such healthcare powerhouses as the North Carolina Healthcare Association (the state hospital) and Vidant Health.
On Wednesday, April 3, the NC House voted to pass the anti-Folwell bill, HB-184 – a bill crafted by the big healthcare players in the state and forced upon the lowly taxpayers by (many) bill sponsors who clearly have ties to the medical field in order to remove NC Treasurer Dale Folwell from his task of fixing the State Health Plan mess, saving the state, state employees and retirees, and taxpayers money, and preventing a financial crisis all so that they can continue over-billing the state through the Plan in order that their status and interests remain strong and well-funded.
HB-184 has one goal and one goal only, despite the title of the bill (“Study State Health Plan Design”), and that is to block implementation of Folwell’s plan and the reforms to State Health Plan.
We’ve all heard the phrases “Too big to fail” or “Too important to fail.” We heard these at the time of the federal bail-out bills, when the federal government stepped in to rescue specific banks and businesses from financial crises. In other words, the government was picking those who it deemed were most important; it was picking and making “winners.” It was this mentality and this action on the part of the federal government, with taxpayer money, that led to the start of the great Tea Party movement – a movement tasked and devoted to constitutionally limited government, fiscal responsibility, and oversight in government to identify abuse and over-reached. The Tea Party seeks nothing more than to ensure that government works as intended, and no more.
When a government becomes more concerned with special interests, then it ceases to be a government “for the people.” When a government is more concerned that hospitals, banks, car manufacturers, and other special interests are shielded from failure (despite their bad management decisions) than making sure the taxpayers are taxed only for those costs and services that touch on their lives and residency in the country or state and when government is more concerned with the financial solvency of those businesses and institutions rather than the financial well-being of its citizens, treating them like an endless source of revenue and nothing more, then it ceases to be a government “for the people.” Gradually, the people become an enslaved taxing class, with hard-earned money going down rat-holes that provide not a single benefit to them. And that’s the threat we are facing should the NC Senate pass HB-184 and this horribly bad bill be signed into law.
The first step, however, has been taken. The NC House has decided to remove Treasurer Dale Folwell completely from his responsibility of straightening out the State Health Plan mess. Reporters and commentators, and opponents of the bill have described the vote on Wednesday as “Dale Folwell losing to NC Healthcare and Vidant Health and other interested healthcare parties. But Folwell perhaps said it best to a reporter: “I didn’t lose anything today. It’s the taxpayers who lost. The taxpayers lost because every dollar that’s unnecessarily spent on health care is a dollar that cannot be spent on public safety, public education, or public roads.” House legislators who voted for the bill clearly did not see the issue in those terms. They cowered to the scare tactics that big healthcare monopolies like Vidant Health might have to close rural hospitals.
State employees, retirees, and taxpayers are not the only ones who have been opposed to this bill. State conservative policy organizations, conservative policy think-tank organizations, conservative talk-radio shows, and conservative journals are united against it as well – the Civitas Institute, the John Locke Society, the Carolina Journal, the County Compass, Wake Up Call (107.1), the Chad Adams Show, etc.
I. BACKGROUND:
A. DALE FOLWELL and the STATE HEALTH PLAN
Dale Folwell enjoys an outstanding reputation, and not only for being an all-around nice guy and a man of utmost integrity. He did an excellent job serving four terms in the NC General Assembly but an even more significant job when he served in Governor Pat McCrory’s administration (2013-2015). Serving as Assistant Secretary of Commerce with the Division of Employment Security, he took the most “broke and broken” unemployment insurance system in the United States and turned it into a national leader in debt-repayment, quality and customer service. This outstanding accomplishment continues to save North Carolina’s employers significant sums annually.
Folwell is known, and rightfully so, as a problem solver.
In December 2015, he resigned from McCrory’s administration to run for the State Treasurer position. The State Treasurer is the keeper of the public purse. In North Carolina, the Treasurer over-sees such big ticket items as the State Pension Plan, from which one in every ten North Carolinians receive a check each month, and the State Health Plan, which for those who do not know, is the state-administered insurance plan used by state employees; it pays for the medical expenses of teachers, state troopers, firefighters, and other state and local employees, and retirees (retired state employees). There are more than 727,000 North Carolina employees alone on the Plan, not including dependents and retirees. The State Health Plan is equivalent in size to the domestic employment base of Amazon, Bircher-Hathaway, and JP Morgan combined.
[To learn more about what the state Treasurer in NC does, check out Dale Folwell’s presentation, “The Price of Promises” – https://www.johnlocke.org/event/the-price-of-promises-2/. He begins talking about the State Health Plan at time 12:30]
When Folwell took office as North Carolina’s Treasurer, he was faced with a crisis concerning the State Health Plan and tasked with solving it. When he ran for the position of Treasurer in 2016, many voted for him expecting him to solve the Plan’s problems as its administration was in the Treasurer’s portfolio. And as soon as he won the election, he immediately went to work to reform the state’s Plan. The State Health Plan is seriously underfunded and currently burdens the state with unsustainable unfunded liabilities (obligations to employees and retirees), and therein lies the crisis. In fact, a recent report by the Pew Charitable Trusts confirmed that NC’s unfunded retirement and health care costs are among the worst in the country. The reality is that the Plan that Folwell inherited is only 5% funded, with $35 billion of the Plan’s liabilities being unfunded. Current spending projections estimate that the Plan will be insolvent by 2023, and unable to pay providers, unless action is taken. Without action, the state Treasurer estimates that every man, woman, and child in the state would have to pay almost $3,200 each to cover our current promises of health care for state and local government retirees.
Just a few days ago (April 4), Folwell gave even more troubling figures. He told the John Locke Foundation that the State Health Plan, which covers 720,000 state employees, retirees, and dependents, is less than 4% funded.
Back in December, Folwell proposed a possible solution – to restructure reimbursement rates for the State Health Plan. His intention was to tie State Health Plan rates to the federally-set Medicare rates, setting reimbursements at up to 235% of Medicare rates, which he calculated would save hundreds of millions of dollars annually. That sounds more than reasonable, yes? Bur for many providers, this would be less than what they currently charge the Plan for their services. A December 2018 NC Health News article on the issue explained, “Hospitals argue that governmental payers such as Medicare and Medicaid both pay less than what it costs to provide care, and so they often depend on commercial payers, such as the State Health Plan, to pay a little more and make up the difference.”
Healthcare prices for the privately-insured, as well as those on the State Health Plan, are higher due to the lower rates paid by Medicaid and Medicare. This essentially means that North Carolinians pay for those programs directly though their state and federal tax dollars, then additionally subsidize the programs through higher insurance prices that are passed on to them by their private or state health insurers. Yet Governor Roy Cooper and some legislators want to add an additional half a million enrollees to North Carolina’s Medicaid program through Medicaid expansion during this current legislative session. House Democratic leader Darren Jackson (D-Wake), for example, said too many patients use hospitals for routine care because they lack health insurance, and so his solution is Medicaid expansion.
Medicaid expansion would likely further compound the financial burden on our state regarding healthcare.
We can start to see what is coming down the road for taxpayers.
Folwell’s plan was/ is called the “Clear Pricing Project” (or “Clear Pricing Plan”) to highlight the fundamental and essential elements of his reform – transparency in the costs of services, procedures, tests, scans, etc and what hospitals charge and establishing a standard formula to use in paying hospitals. The plan, which he planned to launch in January 2020, would require health care providers to publish their prices and not alter or inflate them, thus providing health care consumers pricing information upfront and giving them the opportunity to shop around and compare. The plan would spark competition and ultimately reduce costs. Folwell understands the benefits of a free market type solution.
As Folwell moved forward with his reforms (again, the “Clear Pricing Project” or “Clear Pricing Plan”), NC Healthcare Association and Vidant Health began to push back. The big hospitals claim they will suffer if Folwell’s Clear Pricing Plan goes into effect; they have threatening that if their reimbursements are cut, they may very likely have to close rural hospitals. The scare tactics have been circulated and people are buying into this fake media. On social media and on their website, the Partnership for Innovation in Health Care (PIHC) makes arguments regarding a potential loss of health care jobs if the state implements Folwell’s plan, while claiming that the Treasurer already has transparency in hospital pricing. That last claim, of course, is patently false. In fact, it is the absolute lack of transparency by hospitals in their pricing that led Folwell to suspect that they were not dealing with the State Health Plan honestly and in good faith. And it was the absolute refusal of the hospitals to provide Folwell with pricing information that led the hospitals to seek to have his efforts thwarted and his inquiries stopped and his efforts thwarted. (See later, in the debate from the House floor). Meanwhile, the group that will be most directly affected by any change to the State Health Plan, the State Employees Association of North Carolina (SEANC) has endorsed Folwell’s plan.
The State Employees Association contends that hospitals and other providers have milked the State Health Plan for years by overcharging its members to pay for the health care costs of others – those who are uninsured. Furthermore, it believes the hospitals are being dishonest about their financial situations. SEANC spokeswoman Ardis Watkins doesn’t think hospitals are going to suffer despite their claims. Watkins says: “There’s the facade that nonprofit hospitals operate on a shoestring budget, and that every dollar that comes in for care is spent on care and reinvested in that community. The dark truth is that this razor thin margin they speak of is often the result of hiding their profits in offshore insurance plans and investments overseas, venture capital firms, ACOs, and for-profit telemedicine and software programs.”
The State Employees Association of North Carolina supports Folwell’s efforts. The organization contends hospitals and other providers have milked the State Health Plan for years by overcharging its members to pay for the health care costs of others.
And so, in the hospitals’ decision to frustrate rather than work with the Treasurer, House Bill 184 (HB-184) was born.

B. FOLWELL MODELS the NC STATE HEALTH PLAN AFTER MONTANA’S PLAN – To Save Money
Here is how the NC State Plan (the NC health insurance plan) works: Under the current system, North Carolina contracts with Blue Cross Blue Shield of North Carolina and the company negotiates how much it pays hospitals and doctors for procedures. But those rates are considered confidential. Why? That can’t make sense, or be tolerated, when the Plan is of a contract nature which legally implies complete transparency and a “meeting of the minds.” Besides, when taxpayer money is at stake, there MUST be full disclosure and transparency. As a consequence of the hospitals believing their rates are confidential, Treasurer Dale Folwell doesn’t know how much the state health plan is paying for individual surgeries or doctors’ visits. And the hospitals, as it turns out, aren’t willing to deviate from their position to provide him with that information.
But he does know that the prices are high, inconsistent, and aren’t in line with costs charged by other hospitals. He believes the state is entitled to accountability but he has been unable to get the hospitals on the same page.
The State Health Plan, as mentioned in the previous section, will run out of money by 2023 at which time it will be forced to dip into the general fund. To avert this crisis, Folwell has studied possible solutions (including looking at how other states have dealt with a similar problem) and has come up with an approach which he believes will save the state (and taxpayers) money. Several conservative groups agree with him. This is the Clear Pricing Project, or Clear Pricing Plan, that was mentioned earlier.
According to Folwell, starting in 2020, the state will use Medicare rates as a starting point to decide how much to pay doctors and hospitals for care.
Where did he come up with this plan? Well, it turns out that Montana made a very similar change a few years ago and saved a lot of money.
Alex Olgin explained best, in his article “NC Makes Similar Changes to State Health Plan as Montana” (Oct. 25, 2018), how Treasurer Folwell assessed the State Health Plan problem and came to adopt the Montana solution. In that article, he wrote:
Because Treasurer Folwell doesn’t know how much the state health plan is paying for individual surgeries or doctors’ visits, he’s trying the same approach his counterpart in Montana took a few years ago. The plan sets the rates, and tells doctors and hospitals what it will pay them. Marilyn Bartlett led the change starting in 2014.
At the time, Montana lawmakers said the state health plan needed to get its spending under control for its 31,000 state employees or it would run out of money. Bartlett looked at the data and found the hospitals represented a large part of the spending. She knew she needed to get those costs under control, so she decided to use Medicare rates as a reference point. Bartlett said she offered to reimburse hospitals more than double that amount, which was still less than what some providers were getting paid before. “So we would say I’m not even going to get into the argument that you can’t make a profit or you can at Medicare. There are articles out there that say some hospitals do make a profit and most of them are not-for-profit hospitals,” Bartlett said. “I just said we’re offering more than double that and if that’s not going to work, tell us why. What’s the reasoning?”
Bartlett met a lot of resistance from hospitals, doctors, lobbyists and even some lawmakers. And there were a few holdout hospitals that hadn’t yet signed onto the plan by the time it launched in 2016. But she said all eventually agreed and signed on. That’s because state health plans are so large, they have significant market power.
Bartlett doesn’t know the current cost savings because she now works in a different part of state government, but she projected that within the first 18 months of the change, she saved the state about $16 million. She also said for three years, state employees didn’t have any rate increases.
Marilyn Bartlett was not the state Treasurer or even a state government official. She was brought in, as an insurance insider, to advise the state on how they could reform the state health plan and save money. In a conference room in Montana’s state capital of Helena, she laid out her plan. To her knowledge, no one had ever tried anything like this.
But Bartlett, and Montana’s state government, knew they would be taking on some of the state’s power players: hospitals and health insurers, and their politically-connected lobbyists. If her plan worked, it could create a model for other states and for employers everywhere.
Marshall Allen, in his article, “In Montana, a Tough Negotiator Proved Employers Don’t Have to Pay So Much for Health Care,” wrote:
Bartlett knew employers have negotiating power that few of them use. The health care system depends on the revenue produced by the surgeries, mammograms, lab tests and other services it provides, and it can ill afford to lose it. Bartlett got the job. She would call the industry’s bluff.
The conventional wisdom is that insurance companies want to reduce health care spending. In reality, insurers’ business plans hinge on keeping hospitals and other providers happy — and in their networks — often at the expense of employers and patients.
Employers often feel caught between rising costs and concern that changes they make will be bad for their employees, says Michael Thompson, president of the National Alliance of Healthcare Purchaser Coalitions (NAHPC), which represents groups of employers who provide benefits to more than 45 million Americans. And, he says, they rely on the advice of industry experts instead of digging into the details.
Michael Thompson, president of NAHPC warns: “We have got to get control of this thing or it’s going to bring down the economy, our personal bankrolls and our wages,” he says. “It’ll cost jobs in the United States and it’ll bring down our public programs. This is not a small issue. It’s a huge issue.”
Mr. Allen also explained how entrenched healthcare benefit plans are in this country:
Employer-sponsored health benefits are almost as old as America itself. In 1798, John Adams, the second U.S. president, signed a law that took 20 cents per month from the paychecks of U.S. seamen to fund their medical care. After the Civil War, lumber, mining and railroad companies in the American West withheld money from employee paychecks to pay for doctors and hospitals.
After World War II, such plans became mainstream. Today, about 150 million Americans get their health benefits through their employers. The industry is dominated by what some call the “BUCAH” plans — Blue Cross Blue Shield, UnitedHealth Group, Cigna, Aetna and Humana. Half a dozen health insurers currently sit near the top of the Fortune 500, with combined annual revenue of about half a trillion dollars.
It is very clear why Dale Folwell looked to Montana as the model to fashion reforms to the NC State Health Plan. Not only was its plan going broke (like NC’s plan is), but the insurance carrier (Cigna) that managed the plan and the hospitals were refusing to cooperate with Montana’s state government (exactly as Blue Cross and Blue Shield of NC and NC Healthcare Association and Vidant Health are doing here).
Marshall Allen explains what Ms. Bartlett was up against:
Montana, like many large employers, self-funds its plan. That means it pays the bills and hires an insurance company or other firm to process the claims. More than half of American workers are covered by self-funded plans. As the boss in this arrangement, Bartlett assumed she’d have access to detailed information about how much the plan, which was managed by Cigna, paid for procedures at each hospital. But when she asked Cigna for its pricing terms with the hospitals, Cigna refused to provide them.
Its contracts with hospitals were secret, Cigna representatives told her. That didn’t sit well with Bartlett, she recalls. “The payer cannot see the contract,” she says, “but we agree to pay whatever the contract says we will pay.”
A cumbersome querying process set up by Cigna allowed her to get individual claims and other limited information. But the company would only give her aggregate data, with things lumped together, to show what she paid each hospital. It was like telling a family trying to reduce its grocery spending that it could only see what it spent in a year, not a breakdown of what bread and fruit and other items cost at each market.
When Bartlett continued to demand information, Cigna balked; it needed to balance what she wanted with keeping the hospitals happy. “I don’t see the need for a balance,” she recalls telling them. “I am representing the payer.”
Cigna declined to answer questions about its relationship with Montana’s plan, but it said in a statement that it had prioritized the plan’s preferences and needs.
Bartlett ultimately settled on a radical solution: The plan would set its own prices for the hospitals.
In the illusory world of hospital billing, the hospitals typically charge a high price for a procedure, then give insurers in-network discounts. These charges and discounts might be different for each procedure at each hospital, depending on who has more leverage during negotiations.
The discounts, however, are meaningless if the underlying charges aren’t capped. When Bartlett looked at a common knee replacement, with no complications and a one-night hospital stay, she saw that one hospital had charged the plan $25,000, then applied a 7 percent discount. So, the plan paid $23,250.
A different hospital gave a better discount, 10 percent, but on a sticker price of $115,000. So, the plan got billed $103,500 — more than four times the amount it paid the other hospital for the same operation. Bartlett recalled wondering why anyone would think this was okay.
Under Bartlett’s proposed new strategy, the plan would use the prices set by Medicare as a reference point. Medicare, the federal government’s insurance for the disabled and patients over 65, is a good benchmark because it makes its prices public and adjusts them for hospitals based on geography and other factors. Montana’s plan would pay hospitals a set percentage above the Medicare amount, a method known as “reference-based pricing,” making it impossible for the hospitals to arbitrarily raise their prices.
The situation in North Carolina, as Dale Folwell came to find out, was exactly the same.
Alex Olgin wrote how Treasurer Folwell contacted Ms. Bartlett (a feisty 64-year grandmother) to find out how she came up with Montana’s plan and how she was able to save her state money. The first thing she told Folwell was to “be prepared for pushback.” She was right. She also advised him to be open to hearing from the hospitals. He tried that.
The article explained:
That pushback has already started in North Carolina. The North Carolina Medical Society and the North Carolina Healthcare Association both oppose the plan and say they have other ideas about how to save money. The medical society said in a statement that “radical cost-cutting measures” could negatively impact access to care for state employees.
Treasurer Dale Folwell said providers started receiving information about new reimbursement rates, which on average are 177% higher than Medicare rates. If providers don’t agree to the rates, Folwell said, they’ll no longer be considered in-network.
The state health plan spends over $3.3 billion a year and Folwell estimates these changes will save the plan about $300 million. He acknowledges that some providers will get less, but others — like primary care doctors and mental health practitioners — could see higher reimbursement rates.
The solution to the current State Health Plan problem is that hospitals cannot continue using the Plan as their “endless fund” to recoup the costs they think they are entitled to. The fund is for state employees, their dependents, and retirees ONLY. The hospitals cannot continue to submit rates (confidentially, secretly) in order to keep their institutions fat and happy. The hope is, for Treasurer Folwell, in their final analysis, the hospitals and Blue Cross and Blue Shield will decide it is the “lesser pain” to accept a new contract (the reforms) than to be left out of the deal entirely.
References: Alex Olgin, “NC Makes Similar Changes to State Health Plan as Montana,” WFAE, Oct. 25, 2019, and Marshall Allen, “In Montana, a Tough Negotiator Proved Employers Don’t Have to Pay So Much for Health Care,” ProPublica, October 2, 2018.
 Dale Folwall, NC State Treasurer
Dale Folwall, NC State Treasurer
C. HOUSE BILL 184 (HB-184): “Study State Health Plan Design”
House Bill 184 (HB-184) has as its primary sponsors Reps. Josh Dobson (R-Avery, McDowell, Mitchell), Julia Howard (R-Davie, Rowan), William Brisson (R-Bladen, Sampson), and Gale Adcock (D-Wake). Harry Warren (R-Rowan) was a co-sponsor, and Rep. Greg Murphy (R-Pitt) not only voted to move the bill out of the Health Committee but also voted YES on the House floor. Rep. Donna McDowell White (R-Johnson) was also among the 75 who ultimately voted to pass the bill when it came to a House vote. I mention these representatives for a reason.
HB-184 is legislation essentially crafted by the hospital lobbyists that derails the reform process of the State Health Plan (SHP) and adds up to a billion in unnecessary financial liabilities. Officially titled “Study State Health Plan Design,” the bill deceptively purports to be a “study” bill. The reality is that it is a “stalling” bill, allowing the hospitals to enjoy its current status vis-à-vis the State Health Plan until the 2020 election.
The result of HB-184, as Treasurer Folwell and almost all conservative think-tanks and policy experts agree, would be to would force taxpayers, state agencies, and government employees to pay more to cover higher insurance costs.
The bill has two sections. The first section creates and authorizes the Joint Legislative Study Committee on the Sustainability of the North Carolina State Health Plan to consider how the Plan (the SHP) can be restructured to promote long-term financial health. Clearly, reform is needed: If it continues its current path, the State Health Plan will be unable to pay its debts (ie, “liabilities”) as soon as 2023, which is only four short years away. This insolvency would be catastrophic to the state budget.
Section 1(b) dictates how the Study Committee will be comprised. The Committee is to be comprised of the following ‘voting’ members: four members of the House of Representatives (appointed by the Speaker of the House, who happens to be pro-hospital and against the taxpayer); four members of the Senate (appointed by the President Pro Tempore); the Executive Administrator of the State Health Plan; one member appointed by the North Carolina Medical Society; one member appointed by the North Carolina Healthcare Association; one member appointed by the North Carolina Nurses Association; one member appointed by the State Employees Association of North Carolina; one member appointed by the Retired Government Employees Association of North Carolina; one member appointed by the North Carolina Association of Educators; and one member appointed by the North Carolina Psychiatry Association. The Committee will also include the State Treasurer (Folwell) but he is only an ex officio and has no vote. If it chooses, the Committee may increase its voting membership in any way it thinks best.
Section 2 of the bill prevents the Treasurer and the Board of Trustees for the State Health Plan from making any changes to the provider network or reimbursement rate fee schedule until December 31, 2020. In other words, this section mandates that the current arrangement with third party administrator Blue Cross and Blue Shield of North Carolina continues (unchanged) until that date. This prohibition extends 8 months after the study is concluded, and a full two years into the four-year timeline for the plan’s financial ruin.
Why is the date “December 31, 2020” important? Because that date is after the November election and will give the healthcare lobbyists the chance to get Folwell out of office This bill would block any reforms until the start of 2021, when there may be a new Treasurer – one more aligned with the hospitals and healthcare services.
As you will see below, Rep. Michael Speciale attempted to remove Section 2, but was countered by the bills’ sponsors, explaining that to do so would “gut the bill completely.” So we see the real purpose of the bill…. It’s not really a “study” bill after all. It’s really a stall tactic to maintain the status quo until after the 2020 election, when there may be a new Treasurer. Section 2, together with Section 1(b), is nothing more than a political hit on the office of the State Treasurer.
It should be noted that the actuarial note for the bill estimates that the prohibition on changes will add an additional $1 billion to the state’s $33 billion unfunded liability. Therefore, in addition to delaying a solution to the problem, the bill would add to the state’s liability, and cost by half a billion over the next three years.
As mentioned above, the State Employees Association of North Carolina (SEANC) is the group that will be most directly affected by any change to the State Health Plan. They put their faith in Dale Folwell. This is what the SEANC says about HB-184:
“The legislators [in the NC House] will vote on HB-184 – a bad bill that will cost taxpayers and the State Health Plan members more than $1 million per day if it is enacted. HB-184 was written at the behest of hospital lobbyists to stop Treasurer Dale Folwell from moving forward with SEANC-supported reforms to the State Health Plan. Our initiative – the Clear Pricing Project – will save Plan members $57 million every year in reduced out-of-pocket expenses. It will also save taxpayers more than $258 million annually. Hospitals want to delay these important reforms, and HB-184 would block Treasurer Folwell from implementing the Clear Pricing Project in 2020. Even though the State Health Plan Board of Trustees unanimously approved the Clear Pricing Project last year, hospitals want the General Assembly to ‘study’ the issue for two years. That’s code for ‘let the hospitals keep overcharging for care while we prevent the Treasurer from doing the job he was elected to do.’”
To summarize, HB-184 is a very bad bill. It is bad for state employees and retirees, and bad for North Carolina taxpayers. On the other hand, it is good for the hospitals, good for doctors and nurses, and good for state legislators who are in bed with the hospitals and their lobbyists.
This brings us to the conflicts of interest that surround this bill.
Primary sponsors of HB184 received notable political contributions from the North Carolina Healthcare Association in 2018: Rep. Josh Dobson (R-McDowell County) received $5,200, Rep. Julia Howard (R-Davie County) received $2,000, Rep. William Brisson (R-Bladen County) received $3,000, and Rep. Gale Adcock (D-Wake County) received $6,200. Partnership for Innovation in Healthcare publicly thanked them for sponsoring the bill. Oh, you’ve never heard of this group, Partnership for Innovation in Healthcare? Don’t feel bad… neither did anyone else. With all the new attention given to the State Health Plan and Folwell’s plans to reform it, a new special interest group arrived on Jones Street to peddle influence…. Yep, you got it – the Partnership for Innovation in Health Care (PIHC).
But that’s not all. Several legislators probably should have recused themselves from the vote, being incapable of not giving too much weight to the hospital’s interests. Among such conflicts, these are the more notable ones: Rep Josh Dobson’s wife works at a hospital, Rep. Greg Murphy does his surgeries at Vidant, Reps. Harry Warren and Gale Adcock work at a hospital, and Rep. Donna McDowell White worked in Home Heath.
The Civitas Institute has done some further digging into the conflicts and into the political incentives that may have helped legislators decide to support HB-184. According to an article written by Civitas president Donald Bryson on Friday, April 5 (“State Health Plan Fight: Follow the Money, Part 2”), the critical question to ask is this: Who is the Partnership for Innovation in Health Care ?
Bryon writes in that article:
A glance at the group’s website shows a post office box in Cary: Post Office Box 4449, Cary, NC 27519.
A bit of rummaging at the Federal Election Commission and the State Board of Elections reveals that this is the same post office box used by both the North Carolina Healthcare Association (formerly known as the North Carolina Hospital Association) and the North Carolina Hospital Association Political Action Committee (PAC). It seems that the hospital lobby has very close ties to Partnership for Innovation in Health Care (PIHC).
Bryson then asks the question: “Since PIHC and the North Carolina Hospital Association PAC share a post office box, is there a correlation between legislators that have sponsored HB-184 and political contributions made by the PAC?”
He concludes that there is.
Bryson continues in his article:
According to records from the North Carolina State Board of Elections, of the four primary sponsors on HB184, all four received contributions from the North Carolina Hospital Association PAC. The maximum contribution for state legislative races in 2018 was $5,200 per election. Of the four primary sponsors, which are listed below, two received maximum contributions while the average contribution for the primary sponsors was $3,280.
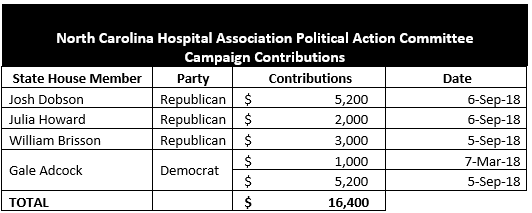
Of the 21 co-sponsors on HB184, 12 received contributions from the North Carolina Hospital Association PAC. Two of the co-sponsors received the maximum contribution, and the average contribution for co-sponsors was $1,762.
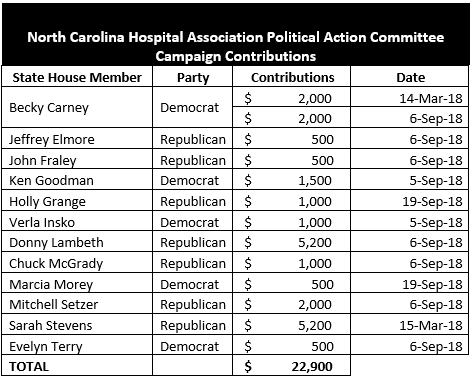
In all, the North Carolina Hospital Association PAC made $39,300 in political contributions to legislators that have signed on to HB184.
Admittedly, there are plenty of legislators who received contributions from the Hospital Association PAC and did not sign on to this legislation but zeroing in on that misses the larger point.
Bryson concludes that there is clear and ample evidence to show that the North Carolina hospital lobby has a great deal of interest in defeating Treasurer Folwell’s plan to reform the State Health Plan.
He then asks a few follow-up questions: (1) Why has the hospital lobby created a shell-organization (the Partnership for Innovation in Health Care, or PIHC) to advocate on its behalf? (2) Why is the hospital lobby opposed to having transparency in their pricing? (3) Why is the hospital lobby fighting pricing transparency on the state health plan while some at the same time lawmakers are proposing a new hospital tax to pay for Medicaid Expansion?
Civitas (Donald Bryson) has done some excellent investigative work and has uncovered some troubling activity on the part of the hospitals and some serious connections between their lobbyist and PAC organization and the legislators who are supposed to be working on behalf of the people. Bryson’s “connecting of the dots” should cause us all to be skeptical of the hospitals’ motives and to feel betrayed by those who sponsored and who voted in favor of HB-184.
Bryson ended his article with this comment: “The Treasurer’s plan is not necessarily a silver bullet, but the unfunded liability is at least 130% larger than our state government’s annual budget. Jones Street needs solutions before we bankrupt ourselves. Meanwhile, expect PIHC and the North Carolina Healthcare Association to retreat to the same tired boogeyman that they use to advocate for Medicaid Expansion and fight Certificate of Need reform – the impact on rural hospitals.”
Reference: Donald Bryson, “ State Health Plan Fight: Follow the Money, Part 2” – https://www.nccivitas.org/civitas-review/state-health-plan-fight-follow-money-part-2/

II. THE HOUSE FLOOR: DEBATE & VOTE (Wednesday, April 3)
It was clear from the start that House leadership, namely House Speaker Tim Moore, was intent on moving HB-184 along very quickly. It went to the Health Committee last Tuesday (March 26) where it passed easily, with only two opposing votes – one from Rep. Phil Shepard (R-Onslow) and the other from Rep. Michael Wray (D-Halifax, Northampton). During the discussion period, Rep. Shepard spoke in opposition to the bill, saying: “Constituent feedback is 2-1 against this bill. There’s a lot of unanswered questions for me and a lot of my constituents. Why the rush to move this bill? We need time to do a thorough analysis of both sides’ claims.”
After passing out of the Health Committee, HB-184 was then set for the Insurance Committee. But surprisingly it was told to skip Insurance and go straight to the House floor for a vote. It took a week for the bill to move forward from committee to a floor vote.
As mentioned earlier, HB-184 was debated on the floor of the House on Wednesday, April 3 Although it was obvious that the bill would pass in the House, there were some conservative representatives who tried to effectively kill the bill, and their attempts deserve mention.
First, Representative Michael Speciale (R-Craven) offered two amendments to the bill, one targeting Section 1(b) and the other targeting Section 2.
Rep. Speciale’s first amendment would alter the language of Section 1(b) two-fold: First, it would make the State Treasurer (Folwell) a “voting” member on the Study Committee and secondly, it would make it impossible to expand the size of the Committee (which is a tactic used when the “powers that be” don’t like the direction a committee seems to be taking).
This first amendment passed by a vote of 106 to 5.
Rep. Speciale’s second amendment would remove Section 2 completely from the bill. Recall that Section 2 prevents the Treasurer and the Board of Trustees for the State Health Plan from making any changes to the provider network or reimbursement rate fee schedule during “the study period” – ie, until December 31, 2020. In other words, this section mandates that the current arrangement with third party administrator Blue Cross and Blue Shield of North Carolina continues (remains unchanged) until that date. Section 2 also prevents the Treasurer from switching the Plan to using referenced based pricing for medical services to the Plan during the “study period.”
The sponsors of the bill opposed the amendment, asserting that removing Section 2 would “gut the bill.”
That amendment failed by a vote of 88 to 23.
During debate on HB-184, Rep. Larry Pittman (R-Cabarrus) cited a memo from the State Health Plan’s Board of Trustees that projects that the plan will be out of money in 2023, and warns that the State cannot wait on a two year study before it acts. The Memo urges action now. Rep. Pittman talked about how hospital groups were groaning about how burdensome the Treasurer’s planed payment changes would be on them [tie pricing of medical services to 172% over the average that Medicare pays for the same service], yet pointed out how well-funded many hospitals are. To support that claim, Rep. Pittman mentioned that the hospital at East Carolina has given $10 million dollars to fund a stadium.
He also addressed how the hospitals dealt with Treasurer Folwell in bad faith. When Folwell had requested payment schedules from the hospital groups, they sent them to him; however, page after page was blacked out. “They might as well have slapped him in the face and spit on him,” Rep. Pittman said.
Pittman also emphasized that the bill would hurt taxpayers but would hit members of the Plan (state employees and retirees) especially hard in that they would have to pay increased premiums and also pay the costs for the unfunded liabilities thru increased taxation. “They would get hit two ways,” he said.
Rep. Pittman called Dale Folwell and “honest” and “competent” man and urged his fellow legislators to “Defeat this bill.”
Rep. Michael Speciale got up to speak again, this time to give his reasons why the bill should be voted down. He said, “We’re told that if we don’t pass this bill, the sky will fall; we’ll lose our rural hospitals.” He said that they’d heard the same thing when he was trying to get rid of the CON [Certificate of Need] laws. “That effort to get rid of the CON laws failed, but nevertheless, shortly thereafter, Vidant closed one of the hospitals in my district anyway.”
“I hear fake news ads” [on the topic of rural hospitals closing if HB-184 doesn’t pass] when I drive in my district,” he said.
Rep. Speciale, as Rep. Pittman before him did, went on to explain how the hospitals dealt with Treasurer Folwell dishonestly and in bad faith. Folwell met with those who are opposing him [mainly large hospital groups] and asked them ‘How much waste, fraud, and abuse is there is in the system?’ The answers they give him ran from 12% to 25%, and so he asked them to figure out how they could reduce costs by 15% (the number he chose from the range they gave him, deliberately intending for there to be as little waste, fraud, and abuse as possible) and said that they needed to get together again as soon as that was done. After that meeting, Treasurer Folwell tried to set follow-up meetings with the hospitals, and time after time he was given excuses why they could not meet with him.
Rep. Speciale continued, “Now we’re faced with $33 to $36 billion dollars in unfunded liabilities. If we don’t allow him to cut costs, how are we going to cut costs because it’ll be on us!”
As to the fears that rural hospitals would be closed if Folwell were allowed to go forward with his reforms, Rep. Speciale said: “Dale Folwell has increased what would be going into rural hospitals. He’s compromised, but they won’t budge an inch. If we do not pass this bill, then the hospital lobby will sit down and talk to him. Let the state Treasurer do what he was elected to do. Throw the politics aside and vote NO !”
Rep. Keith Kidwell (R-Beaufort) also got up to speak in opposition to the bill. He said, “For the last 10 years, health care costs have gone up and up. We asked Treasurer Folwell to handle it. Let’s not bobble him, or we’ll be faced with taking $235 million to $509 million [dollars] from the general fund to deal with the problem AND $1.1 billion will be added to the unfunded liability. HB-184 will cost us a ton of money. We need to cut through partisanship and look at the numbers. We HAVE to block this bill !”
In spite of the arguments and some inconvenient truths, HB-184 (as amended by Rep. Speciale) passed 75 to 36, and it will now be sent to the NC Senate where it is hoped that the bill will be defeated.
The Republican members of the NC House who voted IN FAVOR of the bill are:
Lisa Stone Barnes; John Bell (Greene, Wayne, Johnston), James Boles Jr., William Brisson, Jerry Carter, Kevin Corbin, Ted Davis Jr. (New Hanover), Jimmy Dixon (Duplin, Onslow), Josh Dobson, Jeffrey Elmore, John Faircloth, John Fraley, Holly Grange (New Hanover), Bobby Hanig (Currituck, Dare, Hyde, Pamlico), Cody Henson, Craig Horn, Julia Howard, Chris Humphrey (Pitt, Lenoir), Frank Iler (Brunswick), Steve Jarvis, Donny Lambeth, David Lewis, Chuck McGrady, Greg Murphy (Pitt), Larry Potts, Wayne Sasser, Mitchell Setzer, Carson Smith, Sarah Stevens, John Szoka, John Torbett, Rena Turner, Harry Warren, and Donna McDowell White.
Those who voted AGAINST the bill (Republican and Democrat) are:
Democrats: Reps Terence Everitt, Elmer Floyd, Charles Graham, Joe John, Carolyn Logan, Nasif Majeed, William Richardson, Raymond Smith, and Michael Wray.
Republicans: Jay Adams, Hugh Blackwell, Mark Brody, Dana Bumgardner, George Cleveland (Onslow), Debra Conrad, Ed Goodwin (Bertie, Camden, Chowan, Perquimans, Tyrrell, Washington), Destin Hall, Kyle Hall, Jon Hardister, Pat Hurley, Brenden Jones, Keith Kidwell (Beaufort), Pat McElraft (Carteret, Jones), Allen McNeill, Larry Pittman (Cabarrus), Michelle Presnell, Dennis Riddell, David Rogers, Stephen Ross, Jason Saine, John Sauls, Phil Shepard (Onslow), Michael Speciale (Craven), Larry Strickland; Larry Yarborough, Lee Zachary
House Speaker Tim Moore did not vote.
[If you’d like to hear the whole debate, you can go to the NC General Assembly website (www.ncleg.gov). NC House sessions are archived].
If you are OPPOSED to this bill and do NOT want the NC General Assembly to pass it, make sure you CONTACT YOUR STATE SENATOR ASAP !!
Contact information is available from the NC General Assembly website – www.ncleg.gov.
III. CONSERVATIVE POLICY THINK-TANK GROUPS and OTHER CONSERVATIVE GROUPS STRONGLY OPPPOSE HB-184
As mentioned earlier, state employees, retirees, and taxpayers are not the only ones who have been opposed to this bill. State conservative policy organizations, conservative policy think-tank organizations, conservative talk-radio shows, conservative journals, conservative bloggers, and grassroots conservative groups are united against it as well. They are doing their best to counter the lies, deceptions, and scare tactics being told by the big wealthy hospitals, the Partnership for Innovation in Healthcare, other lobbyists and interested groups and present the truth and the reality to those who will ultimately be burdened with HB-184 and the increased costs incurred by not allowing Treasurer Folwell to enact meaningful changes and reforms to the system.
The Civitas Institute, for one, thought the bill so bad and so burdensome to the inherent right of the people to keep as much of the money they earn as possible (News flash, folks – this is called “fiscal conservatism.” Allowing people to keep the money they earn, reducing taxes, being fiscally responsible – these are essential and core principles of conservatism) that it decided to take as strong a public stand as it could. Besides the many articles it has written outing HB-184 for the bad bill it is, and besides the comments and advice its policy experts have given to those around the state about it, Civitas decided to include the bill in its “grading system.” Civitas grades each North Carolina legislator for “conservatism” in his or her voting record and makes their results available to the public. Conservative organizations, church groups, and voters rely on Civitas’ ratings when they consider which candidate to help promote, or to vote for, and those legislators who seek to hold on to their seats often are conscientious of their rating in order to win re-election. How Civitas rates a legislator matters. The grading will either bolster or detract from their overall “conservative” rating.
Here is Civitas’ position on HB-184 (per president Donald Bryon’s statement):
Elected by the citizens of North Carolina, the State Treasurer SHOULD be allowed to explore solutions to current problems with the State Health Plan, consistent with his statutory and constitutional authority. Instead, HB 184 gives power to a study committee that primarily consists of special interest groups with monied interests in maintaining a lucrative State Health Plan at the expense of taxpayers – namely the North Carolina Healthcare Association (formerly the North Carolina Hospital Association).
The State Health Plan, as currently structured is unsustainable. Years of inaction cannot be rectified through continued inaction. The General Assembly may wish to study an issue on which it may desire to take future action. It is fiscally irresponsible, however, to waste two years with no corrective action when there are only four years until the State Health Plan is fiscally insolvent.
As long as the reform process is derailed, and corrective actions are prohibited by HB-184, the vote to defend freedom is NO.
Civitas Action intends to grade any vote regarding HB-184 in the House or Senate.
Just as Civitas is holding House legislators accountable for their votes on HB-184, it will do the same for NC Senator as well.
While Civitas and John Locke are doing their part in getting the truth out, while talk-radio personalities are doing their best on air to get the truth out, and while conservative writers and bloggers are using their pens to get the truth out, some of the most vocal and powerful commentary is coming from taxpayers and from those who are state employees. For example, Jonathan Merritt, a state employee and activist in Onslow County put a post on social media that is getting a lot of attention. He wrote:
Unlike many who are posting in favor of HB-184 and claim to know what they are talking about, I really DO understand how insurance works. But what everyone seems to be overlooking is that insurance thru the State Health Plan is a benefit that is offered to STATE EMPLOYEES only – as part of a package that allows them to accept positions of employment at a much lower salary than in the private sector. I will give you an example: I work for the state for just over $60,000/year. I left the private sector for this particular state job for reasons that include my age, family concerns, work environment, schedule, and benefits (including healthcare). If I left to go back to the private sector, I would be paid $80,000 – easily, or if I chose to be self-employed, I might be able to earn over $100,000. But in the private sector I wouldn’t get the same excellent healthcare plan and as a self-employed family man, I’d have to pay handsomely for such a plan.
If, as those legislators who support HB-184 would have it, I am being hit to provide others a lower premium or less out-of-pocket costs, at what point does it become more feasible to leave state employment and go back into private or self-employment?
These benefits to state employees are contracted. They aren’t contracted to the uninsured. If the State Health Plan is being raided to compensate for other insurers and/or to compensate for non-payment, or to cover the expenses of those not insured, then the state will quickly lose its resources. Otherwise, individuals will no longer see being a state employee as beneficial.
Again, check out Dale Folwell’s presentation on the State Health Plan and the State Pension Plan, “The Price of Promises” – https://www.johnlocke.org/event/the-price-of-promises-2/ . He begins talking about the State Health Plan at time 12:30 ]
IV. CONCLUSION
HB-184 is a bad bill. It is bad for North Carolina. It is bad for state employees and retirees (including current and retired teachers, firefighters, state troopers, and many more). And it is bad for taxpayers. It is not only bad in what it seeks to achieve (to put big hospitals in a position of power in addressing the State Health Plan) but it is bad in what it does to achieve that goal (removing the office in charge of the Plan, the State Treasurer – Dale Folwell, completely from that task). We shouldn’t put up with such duplicity.
To summarize the situation in a nutshell: State Treasurer Dale Folwell has come up with a plan, the Clear Pricing Plan, to control costs in the State Health Plan. Taking effect in 2020, it would change reimbursement rates on the State Health Plan and implement a reference-based pricing model. In other words, there will be no more price gauging and no more inflating costs to the Plan by hospitals to make up for losses incurred by non-state employees (ie, those receiving healthcare without insurance, including illegals). New legislation, HB-184, was quickly introduced in the NC General Assembly for one purpose only – to block implementation of Folwell’s plan. It passed the NC House on Wednesday, April 3 and has already been sent to the NC Senate.
By trying to take authority away from Dale Folwell, the duly-elected state Treasurer tasked with managing the State Health Plan (and the State Pension Plan), for purely political and self-interested reasons, the powers that be (the big state hospitals, their lobbyist groups, and the legislators in bed with them) are attempting a political coup, with free access to everyone’s pocketbook as the goal. Make no mistake, HB-184 is all about picking “winners and losers” in North Carolina. The hospitals are determined to be the winners and we the taxpayers and state employees and retirees will be the losers.
The State Employees Association of North Carolina does not understand why the hospitals and why state legislators are so opposed to the rightful and reasonable expectation of transparency and accountability in how taxpayer money is spent with respect to the State Health Plan. Why are they so opposed to Treasurer Folwell continuing in his effort (a responsibility specifically tasked to the State Treasurer) to reform the failing Plan and to saving everyone money? SEANC spokeswoman Ardis Watkins commented: “It seems like the most traditionally American thing there is to demand that our government not be irresponsible with tax dollars or support monopolies that hurt the working people of this country.”
I want to end this article by re-emphasizing what Donald Bryson, president of Civitas wrote in his article “State Health Plan Fight: Follow the Money, Part 2.” He wrote: “The Treasurer’s plan is not necessarily a silver bullet, but the unfunded liability is at least 130% larger than our state government’s annual budget. Jones Street needs solutions before we bankrupt ourselves.”
We have to nip this bad bill in this bud. We must take back the control we have over our purses and the finances of our state and not buy into the argument that big business/ big hospitals and special interests should substitute themselves for our places at the table. We MUST share this information with our friends and family. We must get the word out about HB-184. We MUST contact our state senators and tell them to vote NO on the bill. Because the next fight in the General Assembly this session is going to be about Medicaid expansion about how we will have to pay for that.
CONTACT YOUR STATE SENATOR & TELL HIM OR HER TO VOTE “NO” ON HB-184.
References:
Alex Olgin, “NC Makes Similar Changes To State Health Plan as Montana. How Did It Work There?,” WFAE, October 25, 2018. Referenced at: https://www.wfae.org/post/nc-makes-similar-changes-state-health-plan-montana-how-did-it-work-there#stream/0
Marshall Allen, “In Montana, a Tough Negotiator Proved Employers Don’t Have to Pay So Much for Health Care,” ProPublica, October 2, 2018. Referenced at: https://www.propublica.org/article/in-montana-a-tough-negotiator-proved-employers-do-not-have-to-pay-so-much-for-health-care
Raynor James provided the information for the Section on “The House Floor Debate & Vote.” She listened to the audio of the debate on the House floor (I did not, although I spoke with Rep. Speciale, Rep. Pittman, and Rep. Kidwell the day before the vote)
“The Price of Promises,” The John Locke Foundation, February 11, 2019. Referenced at: https://www.johnlocke.org/event/the-price-of-promises-2/ [Dale Folwell gives a presentation here on the problems and liabilities presented by the State Health Plan]
Dan Way, “Bill Blocking State Health Plan Changes Passes 1st Committee Test,” Carolina Journal, March 27, 2019. Referenced at: https://www.carolinajournal.com/news-article/bill-blocking-state-health-plan-changes-passes-1st-committee-test/
Spencer Hardison, “Conservatives Rage Against NC House Republicans Handcuffing State Treasurer Folwell’s Transparency Reforms,” First in Freedom Daily, March 26, 2019. Referenced at: https://firstinfreedomdaily.com/conservatives-rage-against-nc-house-republicans-handcuffing-state-treasurer-folwell-transparency-reforms/
Donald Bryson, “The State Health Plan Fight: Follow the Money, Part I,” Civitas Institute, April 4, 2019. Referenced at: https://www.nccivitas.org/civitas-review/state-health-plan-fight-follow-money-part-1/
Donald Bryson, “The State Health Plan Fight: Follow the Money, Part 2,” Civitas Institute, April 5, 2019. Referenced at: https://www.nccivitas.org/civitas-review/state-health-plan-fight-follow-money-part-2/
Diane Rufino, “North Carolina’s “anti-Folwell” Bill, HB184, Causes Tempers to Flare on Both Sides,” forloveofgodandcountry blog, March 27, 2019. Referenced at: https://forloveofgodandcountry.com/2019/03/27/north-carolinas-anti-folwell-bill-hb-184-causes-tempers-to-flare-on-both-sides/
Diane Rufino, “To Support NC Treasurer Dale Folwell or Not to Support Him – That is the Question for the NC General Assembly,” forloveofgodandcountry blog, March 25, 2019. Referenced at: https://forloveofgodandcountry.com/2019/03/25/to-support-nc-treasurer-dale-folwell-or-not-to-support-him-that-is-the-question-for-the-nc-general-assembly/
Leah Byers, “State Health Plan Debate Shines Light on Medicaid Expansion,” Civitas Institute, December 13, 2019. Referenced at: https://www.nccivitas.org/2018/state-health-plan-debate-raises-concern-medicaid-expansion/
Brant Clifton, “#ncga: Anti- Folwell Lynch Mob Tried to Hide the Facts. (We Found Them!),” The Daily Haymaker, March 25, 2019. Referenced at: http://dailyhaymaker.com/?p=23074

Pingback: Strike HB-184 – CCTA